Patient Education :
WHAT ARE UTERINE FIBROIDS ?
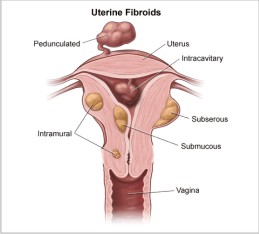
FIBROIDS ARE TUMORS that arise within the muscle of the uterus forming round masses. Some women have single fibroids as large as a football, others have multiple ( up to 20 or more ) which vary in size from a peanut to golf balls and larger.

|
|
Fibroids are named according to their position in relation to the uterine muscle and cavity.
WHAT PROBLEMS DO FIBROIDS CAUSE ?
No Symptoms : Most fibroids up to the size of an orange(12 weeks pregnacy) cause no symptoms. Their mere presence is not a reason to treat them.
Submucus : They protrude into the uterine cavity and cause menstrual cramps, heavy periods, infertility and repeated miscarriages. The diagnosis is made by hysterosonography or hysteroscopy.
Intramural : These fibroids are within the muscle of the uterus and can be very large. Because they enlarge the cavity of the uterus they can also cause heavy periods. The most common problem is PRESSURE symptoms on the bladder and rectum.
Subserous : These are external to the uterine muscle and are connected by a thin stalk. TORSION (twisting) is a complication of subserous fibroid
Degeneration : Rarely there is liquifaction and bleeding within the center causing pain and fever. Infection may also occur. The most common occurrence is during pregnancy.
Fibroids and Infertility, Miscarriage
Only submucus fibroids cause repeated miscarriages. Large intramural fibroids may be the cause of longstanding infertility if all other causes have been excluded.
TREATMENT
Nonsurgical : Fibroids shrink at the menopause to 50% of their size but never go away. GnRh agonists e.g. Lupron, Synarel, Busarelin are medications given by injection or nasal spray that create a temporary menopause allowing shrinkage. However on stopping medication the fibroid regrows to its original size. Therefore longterm treatment is not indicated as these drugs cause severe menopausal symptoms and osteoporosis. They are used for 1-3 months before surgery to reduce the blood loss of surgery.
Surgical : The treatment for removing the fibroids from the uterine muscle is known as MYOMECTOMY. It is a specialised operation done by specialists who have considerable experience in preserving the uterus for future fertility. Hysterectomy should not be a complication of this surgery in experienced hands. It is important that the uterine lining be not entered to allow normal birth later, and that the muscle is adequately repaired in many layers. This operation is traditionally done through a LAPAROTOMY via a 'bikini' or 'up and down' incision. When the fibroids are less than 5 and less than 18 weeks size LAPAROSCOPIC myomectomy can be performed. There are fewer doctors who can perform this than by laparotomy as the need to accurately suture the muscle laparoscopically which is a difficult skill. Inadequate suturing has led to reports of uterine rupture in pregnancy and labour.
Laparoscopic Myomectomy : The advantage of this is that patients can go home the same or next day and be back to work in 1-2 weeks. However it is important that the surgery be as complete as by laparotomy or any advantage is lost. Our center has pioneered the technique of DEEP LAYERED REPAIR of the muscle by laparoscopic suturing. This creates a strong repair allowing normal VAGINAL delivery even after removing larger intramural fibroids. The use of an electric morcellator to remove the fibroid tissue in long strips has made the surgery speedier so that 18 week size fibroids can be treated in 2 hours.It does not matter whether the fibroids are removed by laser, harmonic scalpel, knife or electrosurgery. The skill of the surgeron is paramount to results.
Hysteroscopic Myomectomy : Submucus fibroids are removed by inserting a hysteroscope through the vagina and an electrical loop is used to removed the protruding part. This is rapid and effective surgery without the need of laparoscopy. Estrogen is used after surgery to promote uterine lining regrowth.

|
Large anterior fibroid distorting in front of uterus. |

|
Whitish fibroid in between fallopian tube and uterus. |

|
The anterior fibroid has been removed sparing the uterine cavity. Laparoscopic repair is started. |

|
The anterior fibroid has been removed sparing the uterine cavity. Laparoscopic repair is started. |

|
Completed repair of pictures 1,3. |
A laparoscopic hysterectomy is a minimally invasive surgical procedure to remove the uterus. A small incision is made in the belly button and a tiny camera is inserted. The surgeon watches the image from this camera on a TV screen and performs the operative procedure. Two or three other tiny incisions are made in the lower abdomen.
 Some women do not have their ovaries removed when they undergo a hysterectomy. If the ovaries stay inside, the woman does not need to take any hormones after the surgery and she does not have hot flashes. Some women remove their ovaries because of family history of ovarian cancer or they have an abnormal growth on their ovary.
Some women do not have their ovaries removed when they undergo a hysterectomy. If the ovaries stay inside, the woman does not need to take any hormones after the surgery and she does not have hot flashes. Some women remove their ovaries because of family history of ovarian cancer or they have an abnormal growth on their ovary.
If the woman wants to be 100% certain that she will never menstruate again, she needs to have the entire uterus removed. If the patient has a history of pre-cancerous changes of the cervix or uterine lining, she should have the entire uterus removed. If the operation is being done for endometriosis or pelvic pain, many doctors think the chances for pain reduction are better if the cervix is removed.
Hysterectomy is the surgical removal of the uterus and is performed when a woman has health problems related to it after her child bearing is complete (ideally aged 40+ years).
Symptoms :
Severe pain
Bleeding during menstruation
Other damaged organs
Causes :
The presence of fibroids
The prolapse of the uterus (where the Uterus is shifted from its usual position)
Endometriosis (Presence of the uterus lining in nearby organs which causes pain and bleeding)
Uterine or cervical cancer
Solution :
In most cases, the surgery is done through a tiny incision in the abdomen except in a few exceptional cases where the uterus is so large that there isn't enough room to insert the laparoscopic equipment
In the hysterectomy, the uterus and the surrounding supportive tissue are separated with special tools which maximize efficiency while minimizing blood loss and time of surgery
The uterus is then removed through the birth canal, or, in special instances, by morcellation.
After hysterectomy, a woman will no longer have her periods